By Maggie Zhou, PhD (genetics)
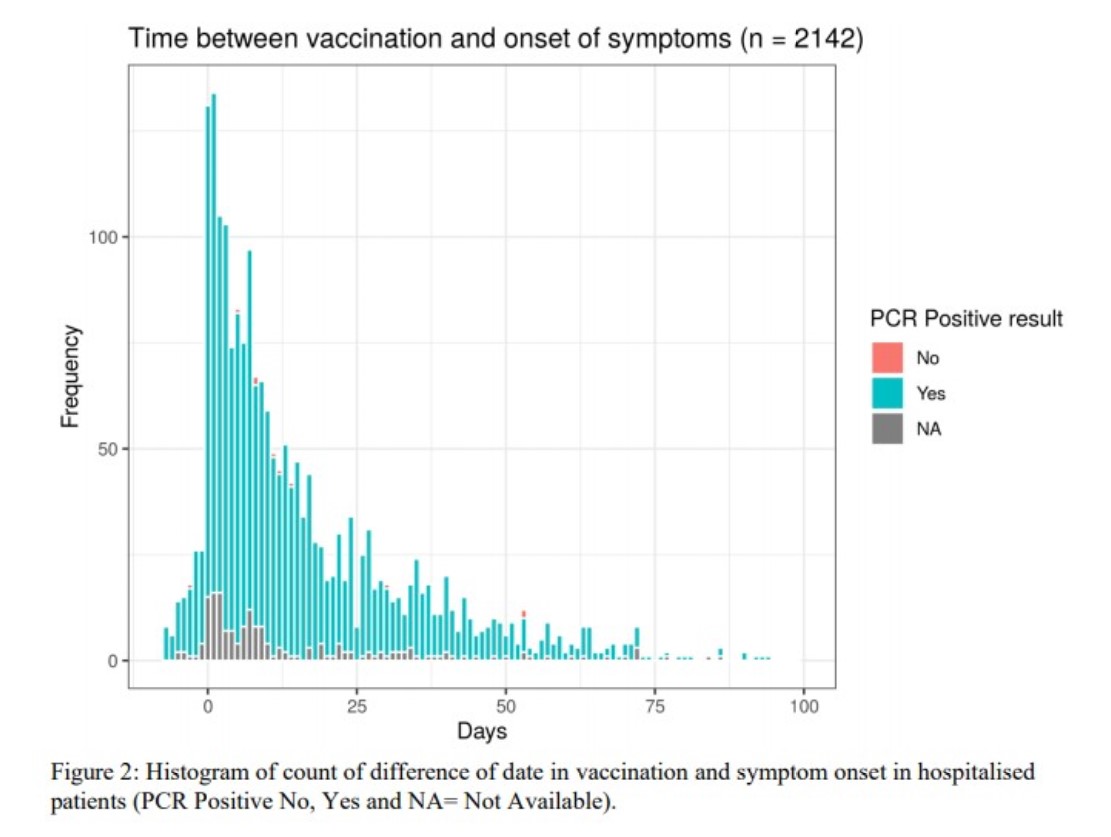
A study on UK government’s website, dated
Apr 2021, conducted by the ISARIC4C consortium, found that among the hospitalized COVID
patients who had ALREADY BEEN VACCINATED, the onset of symptoms is most
commonly from the day of vaccination to 3 days after that. The onset is 5x as frequent ON the day of the
vaccination as the day BEFORE vaccination! [1]
The
preferred mainstream explanation is blaming behavioural
change – they assume that those who had been vaccinated shielded &
isolated less. Yet they have no evidence
to back that up. Crucially, “No one is
suggesting there was a change of behaviour within care homes, except for
inviting people in to carry out the vaccinations. However, care homes in every
corner of the country saw outbreaks from December”, wrote a rebuttal published in the British
Medical Journal.[2]
The other
idea offered by some mainstream academics is that going
to the vaccination centers itself may be a “super-spreader event” - but
again, care homes didn’t fit that bill.
Also, even
if these people did contract the virus on the vaccination day, why would more
of them have symptom onset on that day and the 3 days immediately after, rather
than the usual incubation period of 5 days?
FAR MORE
LIKELY are the following mutually non-exclusive mechanisms:
1. The rebuttal in the BMJ mentioned above[2] pointed out that
both Pfizer and AstraZeneca’s trials had shown white blood cell depletion
in the first 3 days post vaccination.
The phenomenon is known for other vaccines as well, and there’s at least
evidence in children that such transient white cell
depletion results in susceptibility to viral infections.[3] In this scenario, an infection previously
kept in check by the immune system could become active when response to the
vaccine depleted circulating white blood cells.
2. The mRNA
and DNA vaccines use nanoparticles to enclose the nucleic acids. There has been an accumulating number of
studies that found that various types of nanoparticles can interfere with the function of our blood cells, and with the coagulation system, shifting
the hemostatic balance, causing deep vein thrombosis (DVT) and disseminated
intravascular coagulopathy (DIC), among other serious complications.[8,9] Also, the mRNA vaccine nanoparticles contain PEG-lipid,
and the the DNA vaccine nanoparticles contain polysorbate 80, both have
been known to be allergenic and found responsible for anaphylactic reactions in
the past.[10]
3. The spike
protein of SARS-CoV-2 alone, introduced intratracheally, as well as
in in vitro experiments, has been shown to damage lung vascular
endothelial cells by downregulating ACE2, and consequently inhibiting mitochondrial
function, triggering reactive oxygen species production, increasing
glycolysis, and extracellular acidification.[11,4]
4. On Dec
9, 2020, BEFORE vaccination rollouts in most countries, Dr. J. Patrick Whelan
MD PhD, formally warned the FDA that, according to multiple lines
of evidence, vaccines using SARS-CoV-2 spike protein (including mRNA and DNA
vector vaccines) may cause microvascular injury to distant organs including the
brain, heart, liver, and kidneys.[5]
He cited
evidence that while “the coronavirus replicates almost exclusively in the
septal capillary endothelial cells of the lungs and the nasopharynx”, “viral
lysis and immune destruction of those cells releases viral capsid proteins (or
pseudovirions) that travel through the circulation and bind to ACE2 receptors
in these other parts of the body…… that not only damages the microvascular
endothelium but also induces the production of many pro-inflammatory cytokines”. He cited evidence that the brain tissues of
those that died from COVID were found to have pseudovirions (spike, envelope,
and membrane proteins) without viral RNA, in the endothelia of cerebral
microvessels, and that injecting just the S1 spike subunit in mice led to
neurologic signs.[5]
5. On Jan
26, 2021, Dr. Hooman Noorchashm emailed the FDA regulators, Pfizer leaders and
the press, to deliver “a warning and a, nearly
certain, prognostication”, that anyone who has had a recent COVID infection (irrespective
of whether they are symptomatic or convalescent) can be expected to have viral
antigens in the endothelial lining of their blood vessels, and that vaccine
triggered antigen specific immune response will target those antigens, and
therefore those tissues, and cause tissue inflammation and damage.[6] In other words, the vaccines will cause
vasculature damage and blood clots in the lungs, as well as damage in the
vasculature of the brain, heart, liver, kidney etc., anywhere residual viral
antigens from a recent infection may be found.
It's
relevant with regard to what Dr. Noorchashm is warning about, to note that Pfizer's clinical trial protocol (on page 41) explicitly excluded
anyone who has had COVID-19 from enrolment.[7]
6. Another
point specifically about the mRNA and DNA vaccines encoding the spike protein,
is raised by Dr. Sucharit Bhakdi, who was for over 2 decades the head of
the Institute of Medical Microbiology and Hygiene, University of Mainz, and
Editor in Chief of Medical Microbiology and Immunology.
He warned that a large part of the injected
mRNA or DNA-containing nanoparticle packets encoding the spike protein will
reach local lymph nodes, and through there, into blood circulation. In the lymph nodes, when they’re taken up by
lymphocytes which then express the spike protein, those cells will be targeted
for destruction by other lymphocytes, (likely accounting for the white blood
cell depletion mentioned in #1 above).
The lymphocytes thus activated will multiply and swarm out of the lymph
nodes to seek out more S protein antigen.
They’ll attack any muscle cells where the S protein is presented (muscle
swelling, pain).[12]
The
nanoparticles that get into the bloodstream will be trapped there. Some will fuse with blood cells, but most
will be taken up by endothelial cell lining the smallest of veins where
blood flows really slowly. The expression
and presentation of the S protein by these microvascular endothelial cells attracts
and activates platelets, which induces clotting. These cells also produce trash during spike
protein production, which he says will be placed outside the cell, and attracts
killer lymphocytes to attack the presenting endothelial cells, damaging
the vascular lining, causing inflammation, and clotting.[12]
7. Many
have been pointing out from the beginning, the very real danger of Antibody
Dependent Enhancement of Disease (ADE), that any SARS-CoV-2 vaccine may
cause. All attempts to develop a vaccine
against the closest human coronavirus, SARS-CoV, had failed in the past two
decades, when vaccinated animal models got more severe disease and died, upon
challenge with the actual virus. All
SARS-CoV-2 vaccines clinical trials have simply not had enough observation time
to allow such a deadly consequence to become apparent, before the vaccine
rollouts were rushed worldwide – and we’re already seeing the beginning of the
onslaught! [13-15]
8. The
SARS-CoV-2 spike protein has also been found to contain high sequence similarity
to 4 human proteins essential for embryonic development, including
Syncytin-1 and Syncytin-2, since February 2020.[16]
This lead Dr. Wolfgang Wodarg and Dr. Michael Yeadon (Pfizer's former
chief scientific officer) to write an urgent petition on Dec 1, 2020, to the European
Medicines Agency, to halt the vaccine rollout due to the possibility that
antibodies against the S protein in vaccinated women may attack these proteins,
preventing the formation of a placenta, and rendering them infertile.[17]
Like all the other warnings, it was completely ignored.
9. Yet
another treachery with the spike protein is its potential ability to cause
prion disease, both by the
protein[45], and by
the mRNA for it contained in Pfizer and Moderna vaccines[46]. Here’s a lengthy
summery of these two papers.[47]
10. As if
all that isn’t bad enough, some scientists (e.g., Dr. Judy Mikovits) have
stated that vaccinated people may shed microRNAs (miRNA) derived from
the genetic vaccines, which could explain the many adverse health effects that
unvaccinated people around those vaccinated are reporting (especially many
women reporting abnormal and extremely heavy menses, even spontaneous
abortions). She says these miRNAs can
spread through air, and easily taken in by another person, which is part of our
normal process of genetic material exchange with our environment.[18]
11. Here's yet another way that making our own cells express the spike
protein via the genetic vaccines can lead to disaster: causing cells expressing
the spike protein and cells that have ACE2 receptor on their surface to
conglomerate, forming something called a "multinucleated syncytia":
"Proteins that mediate fusion between
viral and cellular membranes can in some cases also do so between cells that
express the viral fusion protein and those that express the viral receptor. For
instance, cells expressing the HIV-1 envelope glycoprotein gp160 can form
multinucleated syncytia with cells expressing the HIV-1 receptors CD4 and
CCR5". The 2003 Nature paper went on to demonstrate that "293T cells
transfected with ACE2, but not those transfected with human immunodeficiency
virus-1 receptors, formed multinucleated syncytia with cells expressing S
protein (of SARS-CoV-1)".[19]
12. A peer reviewed paper from MIT published in Apr 2021,[20]
confirmed their earlier pre-print version published Dec13, 2020,[21] that “Reverse-transcribed SARS-CoV-2 RNA can integrate into the genome of
cultured human cells and can be expressed in patient-derived tissues”.
Their results are “consistent with a LINE1 retrotransposon mediated, target-primed
reverse transcription and retroposition mechanism.” Even though with infection of SARS-CoV-2
virus, they detected only subgenomic sequences derived
mainly from the 3′ end of the viral genome integrated into the DNA of the host
cell, in the case of
mRNA vaccines, given that we’re told the S protein gene is the only gene
encoded by the mRNA, which by default is near the 3’ end, and was given
a poly(A) tail and various other features to stabilize it, and given that tens
of billions of copies of this mRNA are injected in one dose, it seems to me
that there’s a good chance similar reverse transcription and retrotransposition
of the S protein gene - the MOST PATHOGENIC gene of this entire virus - could
really occur, as many scientists have warned from the beginning. Once integrated into the genome, the host
could express the S protein in the long term, which would trigger persistent
autoimmune response, causing attack on the cells it has integrated into.
13. A paper published on May 20, 2021 found
detectable levels of the spike protein in general circulation in 3 of 13 Moderna
vaccine recipients, up to 29 days following the first dose. The S1 subunit of the spike protein,
previously found to be significantly associated with
disease severity in
COVID-19 patients, were found in general circulation in 11 of the 13 vaccine
recipients, detectable up to 14 days after the first dose.[22] This strongly supports many of the above
hypothesized mechanisms of how the vaccine induced spike protein may cause
harm.
14. I came
across this wonderful, peer reviewed, comprehensive review
article
titled “Worse Than the Disease? Reviewing Some Possible Unintended Consequences
of the mRNA Vaccines Against COVID-19”.[23]
Two particularly disturbing things they discussed, among many, are:
- Vaccine
shedding. “…there is a plausible process
by which it could occur through the release of exosomes from dendritic
cells in the spleen containing misfolded spike proteins, in complex with other
prion reconformed proteins. These exosomes can travel to distant places. It is
not impossible to imagine that they are being released from the lungs and
inhaled by a nearby person. Extracellular vesicles, including exosomes, have
been detected in sputum, mucus, epithelial lining fluid, and bronchoalveolar
lavage fluid in association with respiratory diseases (Lucchetti et al., 2021).” They also discussed how, as the internet has
recently discovered, that Pfizer’s clinical trial protocol implied that they
anticipated the possibility of secondary exposure to the vaccine, and that they
even suggested two levels of indirect exposure (i.e., if A is indirectly
exposed to B who is indirectly exposed to C who has received the vaccine, the
vaccine might actually affect A as well).
- An
extremely disturbing scenario they described, is illustrated by the example of Bovine
Viral Diarrhea (BVD).
They wrote:
“A unique characteristic of BVD is that the virus can cross
the placenta of an infected pregnant dam. This can result in the birth of a
calf which carries intra-cellular viral particles which it mistakes as `self.’ Its
immune system refuses to recognize the virus as a foreign invasion, and, as a
result, the calf sheds the virus in large quantities throughout its life,
potentially infecting the entire herd. It has become a widespread practice
to identify such carrier calves and cull them from the herd in an attempt to
curtail infection (Khodakaram-Tafti & Farjanikish, 2017).
“It seems plausible that a dangerous situation may arise in the
future where a woman receives an mRNA vaccine for SARS-CoV-2 and then conceives
a child shortly thereafter. The sperm would be free to take up RNA-embedded
liposomes from the vaccine and convert them to DNA using LINE-1. They would
then produce plasmids containing the code for the spike protein which would be
taken up by the fertilized egg through the process described above. The
infant that is born is then potentially unable to mount antibodies to the spike
protein because their immune system considers it to be `self.’ Should that infant get infected with SARS-CoV-2 at any time in its
lifespan, its immune system would not mount a defense against the virus, and
the virus would presumably be free to multiply in the infant’s body without
restraint. The infant would logically become a super-spreader in such a
situation.”
SEVERAL
MORE AUTOIMMUNE TYPE ADVERSE REACTION MECHANISMS:
15. According
to Kanduc & Shoenfeld, originally published online in Apr
2020,[24]
‘Pulmonary surfactant plays a fundamental role in the physiology of ventilation
by lowering the surface tension at the respiratory air-liquid interface within
the alveoli. Excessively high values of surface tension would lead to alveolar
collapse thus making ventilation and gas exchange impossible.’ Human surfactant proteins and associated
regulators are extremely important for lung function.
They found
that SARS-CoV-2 spike glycoprotein shares 24 pentapeptides (5 amino acid long
segments, or 5-mers) with human surfactant proteins, out of which 13 were found
in 52 SARS-CoV-derived immunoreactive epitopes in the database (epitopes are
exposed parts of an antigen that get recognized by the immune system - so these
13 pentapeptides are known to be in immunogenic parts of SARS-CoV spike). This is compared to 19 pentapeptides shared between human
coronavirus HCoV-229E
and the same
collection of human surfactant
proteins analyzed, out of which only 1 was found to be hosted in only one HCoV-derived epitope. Immune cross-reaction against the body’s
own surfactant
proteins would explain why SARS-CoV-2 can cause so much more lung
pathology compared to HCoV-229E which causes common cold and mild infections.
Amazingly, they also analyzed Pneumocystis carinii, a
fungus responsible for aggressive and highly deadly Pneumocystis pneumonia in
immune compromised patients, and found that it contains 17 of the 24
pentapeptides shared between SARS-CoV-2 and surfactant molecules! Did the creators of SARS-CoV-2 bioweapon
borrow some of these autoimmunogenic peptide elements from Pneumocystis carinii in
hopes of beefing up the virus’ ability to impair respiratory function by
causing an autoimmune attack on one’s own surfactant proteins?
Importantly, the authors warned against using
vaccines based on entire SARS-CoV-2 antigens, which would in itself trigger
autoimmune attacks. THIS WAS IN APR
2020! Yet, their advice was ignored by
vaccine manufacturers and regulatory agencies, and the criminal vaccines were
“developed” and unleashed upon the world’s population.
(In fact,
even long before that, other researchers[25] have cautioned that before
considering a protein as a vaccine antigen, special care should be taken in
analyzing the sequence of tissue cross-reactive epitopes in order to avoid
possible future side effects and autoimmune diseases.)
16. An
article first published online in May 2020[26], found that 13 out of 50 human tissue
antigens they tested cross reacted with a monoclonal antibody against the SARS-CoV-2
spike protein (Fig 1 of the article), and again
warned against using the full length spike protein for vaccines.
17. A Sep 2020 article titled “Molecular mimicry between
SARS-CoV-2 spike glycoprotein and mammalian proteomes: implications for the
vaccine”[27], found that SARS-CoV-2 spike glycoprotein shares surprisingly many
6-mer and 7-mer peptides with humans, mice and to a lesser extent, rats, and
not to other animals tested. See Fig 1 in article.
They
remarked: “A massive
heptapeptide sharing exists between SARS-CoV-2 spike glycoprotein and human
proteins. Such a peptide commonality is unexpected and highly improbable
from a mathematical point of view…” “Likewise, the proteomes of the three human
coronaviruses HKU1, 229E, and OC43, which were used as viral controls, have no
or only a few peptides in common with the spike glycoprotein. In this regard,
it seems that the SARS-CoV-2 spike glycoprotein is phenetically more similar
to humans and mice than to its coronavirus “cousins”.”
“Finally,
this study once more reiterates the concept that only vaccines based on
minimal immune determinants unique to pathogens and absent in the human
proteome might offer the possibility of safe and efficacious vaccines…” – a
point resolutely ignored by the developers of ALL COVID-19 vaccines!
18. An April 2021 article titled “Divergent and self-reactive
immune responses in the CNS [central nervous system] of COVID-19 patients with
neurological symptoms”[28], found that cerebrospinal fluid (CSF)-derived
monoclonal antibodies (mAbs) from an individual with COVID-19 target both viral
and neural antigens, including one mAb that reacted to spike protein and neural
tissue. CSF immunoglobulin G (IgG) from 5 of 7 patients with COVID-19 who
had neurological symptoms showed antineural reactivity. This study “suggests a role of autoimmunity
in neurologic sequelae of COVID-19”, and yet again shows why using full-length
spike sequence in vaccines is insane.
19. A July 2020 paper[29] proposed that it’s the binding
of SARS-COV-2 spike protein with soluble ACE-2 (also
called serum or plasma ACE-2, the ACE-2 enzyme
ectodomain that has been cleaved from the cell surface, in a process
called shedding, that
occurs more frequently in hypertension and heart
disease patients), that triggers autoimmune attacks
on the ACE-2 (and possibly on related ACE), and the pulmonary
vasculature damage because of dysregulation of the renin-angiotensin axis, as well as the subsequent severe
course of disease and multi-organ attack in some COVID-19 patients. The authors further developed their theory in
a May 2021 paper[30], following additional related
information that came to light recently.
Soluble ACE2 was found[31] to be the highest ranked
predictor of total death or cardiometabolic diseases in general, and the serum
of critically ill COVID-19 patients was recently found[32] to contain higher levels of
soluble ACE-2.
If they’re
right, then injecting the population with vaccines that put tens of billions of
copies of the very protein that binds the plasma ACE-2 and could trigger
autoimmune chain of events, would mean that the very people with high plasma
ACE-2 levels and at higher risk of a severe COVID-19 infection, are being directly
given the spike protein to trigger the very same reactions, bypassing the
need for an infection!
MORE ON
BLOOD CLOTS:
20. An article
originally published in Apr 2021, in the New England Journal of Medicine,
titled “Pathologic Antibodies to Platelet Factor 4
after ChAdOx1 nCoV-19 Vaccination”[33], linked blood clotting in
AstraZeneca's COVID vaccine recipients to a pathologic immune reaction against
Platelet Factor 4 (PF4).
The vaccine
recipients presenting with thrombosis (blood clots) and thrombocytopenia (deficiency
of platelets in the blood) syndrome showed “striking clinical similarities”[34] to heparin-induced
thrombocytopenia (HIT), a known and serious complication that could result
occasionally from the use of heparin (an anticoagulant that is also produced by
the body) to treat or prevent thrombosis.
In the case of HIT, the use of heparin can trigger the
generation of antibodies against heparin-PF4 complex. In a subset of these patients, the binding of
anti-PF4/heparin antibodies to platelet-associated PF4 produces receptor
cross-linking, which strongly activates platelets, leading to blood clots. A further subset of those patients presents clinical
symptoms of thrombosis and thrombocytopenia.[35]
In the case
of AstraZeneca vaccine recipients that suffered thrombosis/thrombocytopenia, 22
out of 23 (“mostly young, generally healthy”) patients tested positive for
antibodies against PF4, suggesting a similar mechanism of autoimmune
induced platelet activation that triggered blood clotting.[33] Strikingly, “(a)ll the patients had
d-dimer levels at presentation that were much higher than would be expected in
patients with acute venous thromboembolism and are typically seen in patients
with cancer.”
“The
clinical features of this vaccine-induced syndrome are more typical of those
seen in patients with HIT who have early reexposure to heparin, including severe
thrombocytopenia, aggressive thrombosis, and disseminated intravascular
coagulation.”
“Identification
of the mechanism through which the vaccine could trigger the formation of these
pathologic antibodies would require further study.”
21. In a June 11 interview[48]
of Dr.
Peter McCullough by Reiner Fuellmich, Dr.
McCullough said the spike protein appears to cause a unique form of thrombosis,
which is partly hemagglutination, where the spike protein attaches to sialic
acid residues on red blood cells – normally RBC aren’t involved in
coagulation, but here they are. He also
said that Italian doctors had shown that when the oxygen saturation goes down
in the lungs, it was due to microthrombosis (micro-clotting) – in other words, it
was micro-clotting in the blood vessels that lead to oxygen deficiency, not
the impairment of lung function by viral infection as generally thought, in the
patients that these Italian doctors observed.
In the same
interview Dr. McCullough also mentioned that in some women, the breasts become
so inflamed after the COVID-19 “vaccines”, that radiologists couldn’t read the
mammogram, and Dr. McCullough’s hospital had to change mammography criteria
to deal with that!
ANAPHYLACTIC
REACTION TO POLYETHYLENE GLYCOL (PEG):
22. A December 2020 article in the journal Science[36],
discussed how PEG, a component of the vaccine nanoparticles, could trigger
anaphylactic reactions in some people:
‘As much as 72% of people have at least some antibodies against
PEGs, according to a 2016
study led by Samuel Lai, a pharmaco-engineer at the University of North
Carolina, Chapel Hill, presumably as a result of exposure to cosmetics and
pharmaceuticals. About 7% have a level that may be high enough to predispose
them to anaphylactic reactions, he found.’
‘In 1999, while working at the Walter Reed Army Institute of
Research, Szebeni
described a new type of drug-induced reaction he dubbed complement
activation-related pseudoallergy (CARPA), a nonspecific immune response to
nanoparticle-based medicines, often PEGylated, that are mistakenly
recognized by the immune system as viruses.’
Full text
of the Samuel Lai 2016 article: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6512330/
TREMORS,
BEHAVIORAL & COGNITIVE ISSUES, AGGRESSION, ETC:
23. A twitter thread summed up some studies suggesting a
possible mechanism how the Spike protein can cause neurodegenerative illnesses
and behavioral/cognitive issues[37].
Monoamine
oxidases (MAO-A and MAO-B) are enzymes that degrade neurotransmitters, such as
serotonin, dopamine (DA), and norepinephrine (NE), maintaining a fine balance. Through docking and molecular dynamic
simulations, Hok et al found that the Spike Protein of
SARS-CoV-2 binds to MAO Enzymes, with an affinity for MAO enzymes COMPARABLE to
that for its ACE2 receptor.[38] In other
words, the spike protein creates an artificial EXCESS of these
neurotransmitters (and a misbalance of them), by binding to the enzymes that
would normally degrade them.
A 2006 study found that the immediate effects of
known MAO inhibitors appear to be psychostimulant-like, as they
substitute for the discriminative stimulus effects of cocaine.[39]
MAO
inhibitors also increase serotonin. A 2019 NIH study found that increased extracellular
serotonin in the ventral pallidum (VP) and orbitofrontal cortex (OFC) also may contribute
to reward and may underlie cognitive deficits observed in users of cocaine.[40]
(Can people get addicted to these “vaccines” after frequent shots?)
Evidence
from preclinical and clinical studies support an association between monoamine
oxidase-A brain levels and aggression.[41]
Histamine
is also a monoamine, whose breakdown is inhibited by the downregulation of MAO.
According to this page about histamine, “Monoamine Oxidase (MAO) is an
enzyme that breaks down N-methylhistamine to N-methylimidazole acetic acid.
SNPs in the gene that encodes for this enzyme can cause histamine levels to
stay high rather than be degraded.”[42] Interestingly,
a paper in Inflammation Research said “Reports that the
over-the-counter histamine H2 receptor antagonist famotidine could help treat …COVID-19…
appeared from April 2020.”[43]
SUPPRESSION
OF INNATE IMMUNE RESPONSE, DNA REPAIR ETC. BY THE “VACCINES”:
24. An excellent June 2022 paper with Dr. Peter A.McCullough as the
senior author, titled “Innate immune suppression by SARS-CoV-2 mRNA
vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs” reviews
evidence and details the many mechanisms of how the COVID-19 “vaccines” are
able to suppress innate immunity, and cause cancer, neurodegenerative diseases,
and a host of other conditions.[44]
They cited a
study on how the spike transfected cells release exosomes loaded with microRNAs
(miRNA) that suppress USP33 and IRF9 levels in distant cells/tissues, while activating
a range of pro-inflammatory gene transcripts.
IRF9 is a interferon regulatory factor, critical in interferon (IFN)
mediated innate immunity.
They cited
a Chinese study that found volunteers who received the inactivated whole SARS-CoV-2
“vaccine” had increased NF-κB signaling and reduced type I IFN responses 28
days after “vaccination”.
They cited
studies that found the spike protein is able to both directly inhibit DNA
repair in transfected cells (with implications on cancer, and adaptive immunity
which is dependent on NHEJ recombination), and indirectly by changing the miRNA
content of exosomes released by transfected cells, thereby inhibiting DNA
repair mechanisms in distant cells and tissues that take up these exosomes.
They also
showed how the methods used by mRNA “vaccine” designers to stabilize the spike
mRNA, including the high GC content, and especially the potential Guanine
quadruplexes (pG4s), may be the culprit in initiating prion-like aggregation
and neurological disease onset, as well as in causing cancer; etc. etc.)
So indeed,
the spike protein that the vaccines contain or encode for, is alone sufficient
to cause COVID symptoms (and deaths in severe cases), and have numerous medium
to long term potential serious consequences.
Only criminal governments would have rushed it ahead and imposed it on
the world with utter deceit.
[2] https://www.bmj.com/content/372/bmj.n783/rr
[3] https://pubmed.ncbi.nlm.nih.gov/29525279/
[4] https://medicalxpress.com/news/2021-04-sars-cov-spike-protein-lung.html
https://www.eventscribe.net/2021/EB2021/index.asp?presTarget=1644160
[5] https://www.regulations.gov/document/FDA-2020-N-1898-0246
[7]https://media.tghn.org/medialibrary/2020/11/C4591001_Clinical_Protocol_Nov2020_Pfizer_BioNTech.pdf
[8] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6829615/
[9] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6289228/
[10] https://www.nejm.org/doi/full/10.1056/NEJMra2035343
[11] https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.318902
[12] https://www.goldegg-verlag.com/goldegg-verlag/wp-content/uploads/corona_unmasked_engl_leseprobe.pdf
[13] https://journals.plos.org/plosone/article?id=10.1371%2Fjournal.pone.0035421
[14] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3209347/
[15] https://www.bulatlat.com/2020/08/21/hazards-of-the-covid-19-vaccine/
[16] https://virological.org/t/response-to-ncov2019-against-backdrop-of-endogenous-retroviruses/396
[18] https://jermwarfare.com/blog/judy-mikovits-viruses
[19] https://www.nature.com/articles/nature02145
[20] https://www.pnas.org/content/pnas/118/21/e2105968118.full.pdf
[22] https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciab465/6279075
[23] https://ijvtpr.com/index.php/IJVTPR/article/view/23
[24] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7165084/
[25] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6141484/
[26] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7246018/
[27] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7499017/
[28] https://www.cell.com/cell-reports-medicine/fulltext/S2666-3791(21)00116-6
[29] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7351250/
[30] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8021777/
[31] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7529405/
[32] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7848790/
[33] https://www.nejm.org/doi/full/10.1056/NEJMoa2105385
[34] https://www.hematology.org/covid-19/vaccine-induced-immune-thrombotic-thrombocytopenia
[37] https://twitter.com/Parsifaler/status/1452099036077608963
[38] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8868002/
[41] https://rarediseases.info.nih.gov/diseases/3531/monoamine-oxidase-a-deficiency
[42] https://healinghistamine.com/blog/genetics-histamine-intolerance/
[43] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7673069/
[44] https://www.sciencedirect.com/science/article/pii/S027869152200206X
[45] https://www.mdpi.com/2076-2607/10/2/280
[46] https://scivisionpub.com/pdfs/covid19-rna-based-vaccines-and-the-risk-of-prion-disease-1503.pdf
[48] Video
titled “DR. PETER MCCULLOUGH ON WITH REINER FUELMICH JUNE 11, 2021” https://www.bitchute.com/video/rKP61hruGxIt/
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Maggie Zhou received her PhD in genetics from the University of Wisconsin - Madison in 1997, and worked as a computational biologist for a number of years. She is currently an independent seeker of truth.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~


No comments:
Post a Comment